

Comparison of Causes Symptoms and Treatment of Kwashiorkor and Marasmus
Nutritional deficiencies are a serious global concern, especially among children. Two major forms of severe malnutrition are kwashiorkor and marasmus. Both conditions arise from inadequate nutrient intake but differ in their specific causes, symptoms, and effects on the body. In this article, we will explore the difference between kwashiorkor and marasmus table, discuss kwashiorkor and marasmus symptoms, and understand their causes, treatments, and preventive measures.
What are Kwashiorkor and Marasmus?
Kwashiorkor is a form of malnutrition that primarily occurs due to severe protein deficiency. Children with kwashiorkor may receive enough calories from other nutrients, but the protein intake remains insufficient.
Marasmus, on the other hand, arises from a deficiency of both calories and proteins, along with other essential nutrients such as carbohydrates and fats. This condition is often linked to extreme poverty and chronic food scarcity.
Causes of Kwashiorkor and Marasmus
Kwashiorkor
Severe lack of protein in the diet.
A diet high in carbohydrates but low in protein.
Poor socio-economic conditions and limited access to protein-rich foods.
Marasmus
Deficiency of proteins, calories, and other nutrients (carbohydrates and fats).
Chronic starvation due to poverty, famine, or severe neglect.
Frequent infections that increase the body’s energy requirements.
Difference Between Kwashiorkor and Marasmus Table
Below is the difference between kwashiorkor and marasmus table, highlighting their key distinctions:
Kwashiorkor and Marasmus Symptoms
It is essential to recognise kwashiorkor and marasmus symptoms early to prevent long-term health complications.
Symptoms of Kwashiorkor
Oedema (swelling in the face, feet, ankles, and belly)
Thinning of muscles and limbs
Flaky or patchy skin
A fatty, enlarged liver
Changes in hair colour and texture (hair may become brittle or reddish)
Irritability and lethargy
Symptoms of Marasmus
Extreme weight loss and a very thin, emaciated appearance
Absence of subcutaneous fat
Dry, wrinkled, and loose skin
Stunted growth or reduced height for age
Muscle wasting, leaving children frail and weak
Poor appetite and frequent infections
Treatments for Kwashiorkor and Marasmus
Dietary Management
Kwashiorkor: Emphasise protein-rich foods such as pulses, dairy products, eggs, and lean meats. Gradually introduce balanced meals that include all essential nutrients.
Marasmus: Restore overall calorie intake by including carbohydrates, fats, and proteins in well-planned, frequent meals. Start slowly to avoid metabolic complications.
Medical Supervision
Both conditions may require treatment under close medical supervision.
In severe cases, hospitalisation is needed for intravenous fluids, electrolyte balance, and treatment of underlying infections.
Nutritional Supplements
Ready-to-Use Therapeutic Foods (RUTF) can help manage acute malnutrition.
Micronutrient supplements (vitamins and minerals) support faster recovery.
Prevention
Educate caregivers about balanced diets and the importance of including protein, carbohydrates, and healthy fats in meals.
Encourage breastfeeding and timely introduction of complementary foods.
Implement community programmes to improve food availability and security.
Additional Tips and Unique Insights
Include variety in meals: Consuming diverse food groups ensures a steady supply of macronutrients and micronutrients.
Monitor child growth: Regular check-ups to track height and weight can catch early signs of malnutrition.
Hygiene and sanitation: Good hygiene practices help prevent infections that can worsen malnutrition.
Community support: Charitable organisations and local food banks can aid families in poverty-stricken areas.
Quick Quiz
Which nutrient is mainly deficient in kwashiorkor?
Answer: Protein.
Name a common feature of marasmus.
Answer: Extreme weight loss or muscle wasting.
What causes fatty liver in kwashiorkor?
Answer: The lack of protein impairs the normal transport of fat, leading to its accumulation in the liver.
State one way to prevent marasmus.
Answer: Providing balanced meals that include sufficient carbohydrates, proteins, and fats.
Related Topics:


FAQs on Difference Between Kwashiorkor and Marasmus in Children
1. What is the difference between Kwashiorkor and Marasmus?
The main difference between Kwashiorkor and Marasmus is that Kwashiorkor is caused primarily by protein deficiency with adequate calorie intake, while Marasmus is caused by severe deficiency of both protein and calories.
- Kwashiorkor: Protein deficiency, edema (swelling), fatty liver, distended abdomen.
- Marasmus: Severe wasting, extreme weight loss, no edema, loss of muscle and fat.
- Kwashiorkor often shows swollen appearance due to fluid retention.
- Marasmus shows a very thin, “skin and bones” appearance.
2. What is Kwashiorkor?
Kwashiorkor is a severe form of malnutrition caused mainly by a lack of dietary protein despite adequate calorie intake.
- Common in children after early weaning.
- Characterized by edema, swollen belly, and fatty liver.
- Caused by low levels of plasma proteins like albumin.
- Often seen in regions with protein-poor diets.
3. What is Marasmus?
Marasmus is a severe form of protein-energy malnutrition caused by deficiency of both calories and protein.
- Leads to extreme muscle wasting and fat loss.
- No edema is present.
- Children appear very thin and underweight.
- Results from prolonged starvation or inadequate feeding.
4. Why does edema occur in Kwashiorkor but not in Marasmus?
Edema occurs in Kwashiorkor due to low levels of plasma protein albumin, which reduces osmotic pressure and causes fluid leakage into tissues.
- Protein deficiency lowers blood oncotic pressure.
- Fluid accumulates in tissues, causing swelling.
- In Marasmus, total calorie deficiency prevents fluid retention, so edema is absent.
5. What are the symptoms of Kwashiorkor and Marasmus?
The symptoms of Kwashiorkor and Marasmus differ mainly in swelling and body wasting.
- Kwashiorkor: Edema, enlarged liver, skin depigmentation, irritability.
- Marasmus: Severe weight loss, muscle wasting, sunken eyes, weakness.
- Both conditions show growth failure and increased infection risk.
6. What causes Kwashiorkor and Marasmus?
Kwashiorkor is caused mainly by protein deficiency, while Marasmus is caused by deficiency of both protein and total caloric intake.
- Poor diet lacking essential nutrients.
- Early weaning onto carbohydrate-rich but protein-poor food (Kwashiorkor).
- Chronic starvation or famine (Marasmus).
- Infections that increase nutritional demands.
7. Which is more severe, Kwashiorkor or Marasmus?
Both Kwashiorkor and Marasmus are severe forms of malnutrition, but Marasmus often reflects more prolonged energy deficiency.
- Marasmus: Severe wasting and long-term starvation.
- Kwashiorkor: Higher risk of complications due to edema and liver damage.
- Both can be life-threatening without treatment.
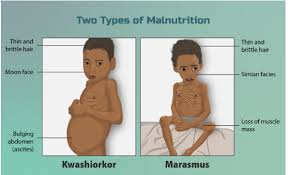
8. How is Kwashiorkor different from Marasmus in appearance?
In appearance, Kwashiorkor shows a swollen body due to edema, while Marasmus shows extreme thinness without swelling.
- Kwashiorkor: Puffy face, distended abdomen, skin changes.
- Marasmus: Prominent ribs, thin limbs, loss of subcutaneous fat.
- Hair discoloration may occur in Kwashiorkor.
9. How are Kwashiorkor and Marasmus treated?
Kwashiorkor and Marasmus are treated by gradual nutritional rehabilitation and medical care.
- Careful refeeding with balanced protein and calorie intake.
- Correction of dehydration and electrolyte imbalance.
- Treatment of infections.
- Monitoring to prevent refeeding syndrome.
10. Can Kwashiorkor and Marasmus occur in adults?
Yes, Kwashiorkor and Marasmus can occur in adults, but they are more common in young children.
- Adults may develop them during famine, chronic illness, or eating disorders.
- Protein deficiency in adults can still cause edema (Kwashiorkor-like condition).
- Severe starvation leads to muscle and fat wasting similar to Marasmus.










